
 Do colonoscopies contribute to Parkinson’s? I was sent this information by one of my readers, Susan, who has been doing quite a bit of research on this topic. I think her findings are interesting and definitely worth keeping an eye on. And perhaps one of you has more information or experience to contribute?
Do colonoscopies contribute to Parkinson’s? I was sent this information by one of my readers, Susan, who has been doing quite a bit of research on this topic. I think her findings are interesting and definitely worth keeping an eye on. And perhaps one of you has more information or experience to contribute?
I have long questioned the safety of colonoscopies, you can download my Colonoscopy Report with all the data (from medical journals) showing they cannot be sterilized. Everyone considering a colonoscopy should push their GI to provide a disposable colonoscope. They are not available in North America yet, but they sure should be! If you do decide to have a colonoscopy, then be sure and follow my protocols for pre- and post-colonoscopy treatment to help protect your colon from damage and infection.
Without further ado, I am turning this post over to Susan…
First, I would like to stress that there is no evidence that colorectal cancer (CRC) screening colonoscopies are spreading Parkinson’s Disease (PD). My concerns are based on publicly available information, and I am not saying anything that is not already available on the internet. Since there are other CRC screening methods, such as FIT, erring on the side of caution may be prudent until the scientific community addresses this issue.
My concerns
I am very concerned about the increasing rates of neurodegenerative diseases, such as Alzheimer’s disease (AD) and Parkinson’s disease (PD).
AD and PD are characterized by a prion-like templated conversion of normal proteins (tau, amyloid beta, and/or α-synuclein) into a pathologic misfolded conformation, and at least 5 papers have suggested that further studies are needed to clarify whether iatrogenic transmission of neurodegenerative disease pathology may be occurring.(1)
If iatrogenic transmission of AD and PD were occurring, it may be difficult to detect. An unknown exposure rate, an unknown infection rate after exposure, and multiple possible transmission routes would require a large dataset.
The Global Burden of Disease (GBD), when used in conjunction with other information, seems to suggest that iatrogenic transmission of PD via CRC screening colonoscopy may be occurring.
The transmission of pathologic α-synuclein from one person to that of another via colonoscopes has been described as theoretically conceivable.
Although persons developing PD may be predisposed to diagnostic colonoscopies, they do not seem to be predisposed to colorectal cancer (CRC) screening colonoscopies.
There are a number of databases (eg. Medicare, Veterans Affairs, Nurses’ Health Study, Electronic Health Records, etc) that may be useful in assessing the risk of PD for persons who had a CRC screening colonoscopy. Comparing the risk of PD for persons who had a CRC screening colonoscopy and those who had a CRC screening fecal test (FIT) may reduce ascertainment bias.
Below is evidence that suggests transmission of PD pathology via colonoscopy may be occurring followed by a biological explanation for why transmission may be possible.
Evidence that suggests transmission of PD:
By looking at population data from the GBD, it can be seen that the changes in PD incidence rates seem to coincide with events expected to affect CRC screening rates.
Events expected to affect CRC screening in the US:
1995 – United States Preventative Services Task Force (USPSTF) first recommended CRC screening for ages 50+ years
2010 – Affordable Care Act (ACA) signed into law
2010 – Centers for Disease Control and Prevention (CDC) received funding from Congress to initiate the Colorectal Cancer Control Program (CRCCP)
2018 – National Colorectal Cancer Roundtable’s Initiative “80% by 2018” end date
Event expected to affect CRC screening in the UK:
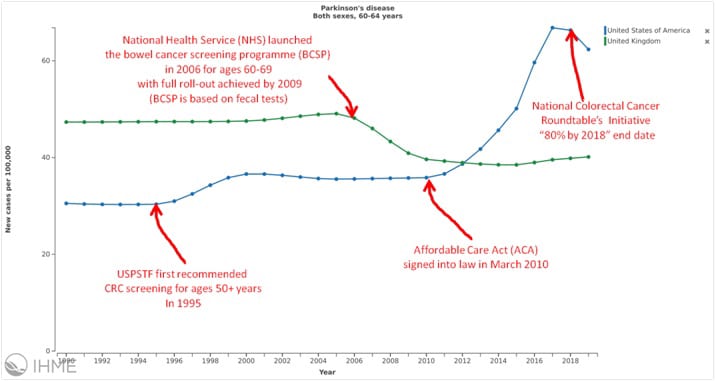
2006 – National Health Service (NHS) launched the bowel cancer screening programme (BCSP) for ages 60-69 with full roll-out achieved by 2009
In the age specific graph (60-64 years) generated by the Institute for Health Metrics and Evaluation (IHME) using GBD data, PD incidence went down in the UK in 2006 and coincides with the launch of the BCSP. The BCSP is based on fecal tests, and the PD decrease may reflect a decrease in opportunistic CRC screening colonoscopy.
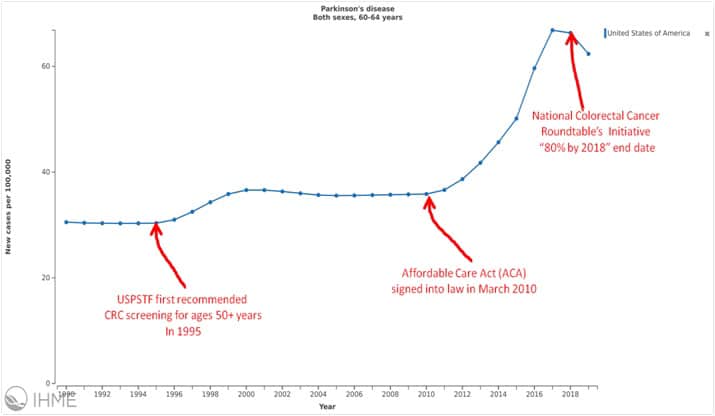
In contrast, PD incidence went up in the US in 1996 after the USPSTF first recommended CRC screening in Dec.1995. The most commonly used CRC screening test in the US is colonoscopy.
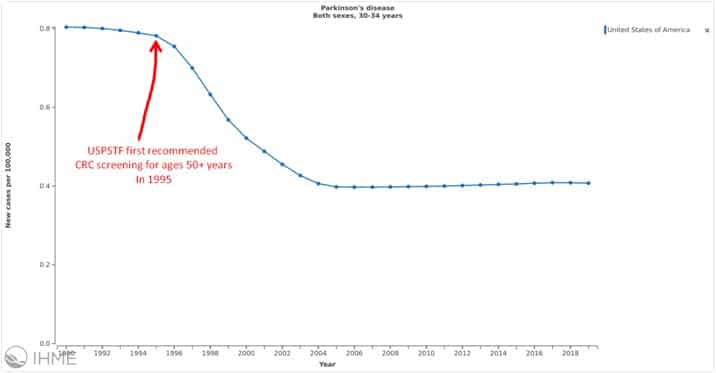
When looking at the different age-specific groups in the US, it can be seen that all age groups under age 50 had a decrease starting in 1996 and the age-specific groups over age 50 had an increase starting in 1996. The PD decrease for age groups under 50 may reflect the expected decrease in CRC screening for these age groups after the 1995 USPSTF recommendation.
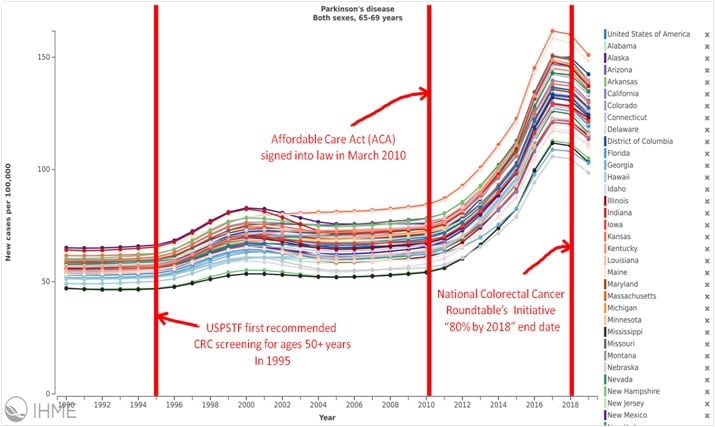
A large rate increase after 2010 can be seen for all 50 US states, and is especially striking, but it is not seen in any of the age groups under 50 years.
Because this rate increase can be seen in all 50 states, it may suggest a nationwide factor, rather than a statewide or regional factor as might be expected with changes in environmental toxin exposure. Although the rate changes seem to coincide with events expected to affect CRC screening usage, other explanations cannot be excluded. One example might be changes to diagnostic criteria.

Additional evidence includes the IPUMS National Health Interview Survey that shows a statistically significant increase in “movement disorder, such as PD” for those who have had a CRC screening exam. There were 48 incidences out of 5,535 people who had a CRC screening exam (0.9; 95% CI =0.7-1.1), vs 40 incidences out of 7,520 people who did not (0.5; 95% CI =0.4-0.7).
The IPUMS data is limited to 2008 as that was the only survey year that included both the CRC screening question and the movement disorder, such as Parkinson’s question.

There is other evidence that also suggests transmission of PD pathology via colonoscopes may be occurring.
The inverse association between PD and smoking is well established by over 70 studies. Whether this association is causal is still debated and may be due to confounding by a covariate of smoking. Several studies have found that current smokers are less likely to participate in CRC screening compared to never smokers. Compared with never smokers, current smokers are less likely to ever have received a colonoscopy. [JAMA Netw Open 2, e193759].
Using data from the IHME and the CDC for the years 2004-2018, the expected inverse association between PD incidence rates and current smoking can be seen at a population level.

However, a stronger correlation can be seen between PD incidence rates and endoscopic CRC screening utilization.

A strong positive correlation between PD incidence rates and CRC screening endoscopy rates can be seen at a population level for the US and for all ten states explored. A MedRxiv preprint describing this is available here.
Additional evidence that suggests colonoscopy may be transmitting Parkinson’s Disease (PD) includes the decreased risk of colorectal cancer (CRC) for PD patients. Persons with PD have a decreased risk of CRC when compared to persons without PD, however, this decreased risk is not seen in persons diagnosed with PD at an age of >75 years [Cancer Epidemiol 43, 9-14; Parkinsonism Relat Disord 35, 42-47]. CRC screening colonoscopy reduces CRC risk by removing precancerous polyps. The USPSTF recommends CRC screening be stopped at age 75. It may be that the inverse association between PD and CRC risk also is confounded by a positive association between PD incidence and CRC screening colonoscopy.
It may be that procedures used to diagnose/treat Inflammatory bowel disease (IBD) are transmitting PD pathology. In Inflammatory bowel disease and Parkinson’s disease: common pathophysiological links [Gut. 2021;70(2):408-417], it was noted that there may be an elevated risk of PD among IBD patients, but IBD risk does not seem to be elevated among PD patients.
Finally, in Prevalence of Prodromal Parkinson’s Disease as Defined by MDS Research Criteria among Elderly Patients Undergoing Colonoscopy it was concluded that “the prevalence of prodromal PD in patients undergoing diagnostic colonoscopies may be higher compared to the general elderly population”[J Parkinsons Dis. 2017;7(3):481-489].
Biological explanation for why transmission may be possible:
Many neurological diseases are characterized by a templated conversion of normal proteins into a misfolded conformation. In the case of PD, misfolded alpha-synuclein protein converts normal alpha-synuclein into the misfolded version. PD pathology has been shown to spread from the gastrointestinal tract to the brain via the vagus nerve [Acta Neuropathol 128, 805-820].
Creutzfeldt-Jakob disease (CJD) is another misfolded protein disease. Transmission of CJD has been shown to occur via contaminated surgical equipment and transplanted diseased tissues. Misfolded CJD proteins adhere to stainless steel and are not be removed during routine sterilization procedures. The World Health Organization (WHO) considers these proteins to be biohazards and has published infection control guidelines for handling contaminated equipment, tissues and fluids.
The misfolded proteins associated with PD and other proteopathies also adhere to a variety of surfaces, are not removed during routine sterilization procedures [Colloids Surf B Biointerfaces 166, 98-107; Sci Rep 8, 10788] and have been found in a variety of tissues and fluids, including the colon [Mov Disord 27, 709-715]. Although precautions are taken when handling the misfolded proteins associated with CJD to prevent iatrogenic disease transmission, similar precautions are not widely practiced when handling the misfolded proteins associated with other proteopathies, such as PD.
For transmission of PD pathology to occur via a colonoscope:
1. αSynPD seeds would need to be present in the colon of a PD patient:
“Clinicopathological evidence suggests that α-synuclein aggregation, the pathological signature of Parkinson’s disease, can be detected in gastrointestinal tract neurons in Parkinson’s disease.” [Mov Disord. 2012;27(6):709-715]
“The presence of LB in the GI tract, not solely α-syn expression, may prove useful, distinguishing neurodegenerative disease patients from normal controls.” [Appl Immunohistochem Mol Morphol. 2019;27(7):543-548]
2. αSynPD seeds would need to adhere to the surface of the colonoscope:
“Oligomeric and fibrillar α-Syn adhere to various surfaces made of plastic, glass, stainless steel, or aluminum.” [J Parkinsons Dis. 2016;6(1):143-151]
“Findings that fibrillar α-Syn can seed the aggregation of monomeric α-Syn both in cell cultures and in animal models, coupled to observations that injected alpha -Syn fibrils propagate from the olfactory bulb, intestine, muscle and the blood to the central nervous system suggest that α-Syn fibrils should be handled with caution in laboratories and hospital settings.” [J Parkinsons Dis. 2016;6(1):143-151]
3. αSynPD seeds would need to remain after colonoscope reprocessing:
(a) Colonoscope reprocessing is not always effective:
“Despite reprocessing in accordance with US guidelines, viable microbes and biologic debris persisted on clinically used gastrointestinal endoscopes, suggesting current reprocessing guidelines are not sufficient to ensure successful decontamination.” [ Am J Infect Control. 2015;43(8):794-801]
“The rates of postendoscopic infection per 1000 procedures within 7 days were 1.1 for screening colonoscopy, 1.6 for non-screening colonoscopy” [Gut 2018;67:1626-1636]
“A number of factors, including lapses in reprocessing, biofilm formation, endoscope design issues and endoscope damage, contribute to gastrointestinal endoscopy associated infection. “[Ann Clin Microbiol Antimicrob.2018; 17, 36]
“Endoscopes cannot be autoclaved because they are made of heat-sensitive materials. There are low-temperature alternatives, including ethylene oxide (EtO) gas sterilisation, which have been adopted in response to culture-positive endoscopes and endoscopy-associated outbreaks.” [Ann Clin Microbiol Antimicrob.2018; 17, 36]
(b) Ethylene oxide is insufficient for PrP prions (CJD) :
“Providing the medical instrument is heat resistant, an autoclave cycle at 134°C for 18 minutes or more is generally effective for prion inactivation. For heatsensitive instruments, such as endoscopes, hydrogen peroxide gas plasma sterilization using Sterrad NX is recommended. Ethylene oxide inactivates prions to log 3 or less, which is insufficient for medical applications.”[Curr Issues Mol Biol. 2020;36:23-32]
(c) Even if methods effective for PrP are used, they may not be effective for αSynPD seeds:
“We previously showed that methods designed to decrease PrP prion infectivity that are based on the use of sodium hypochlorite (20,000 ppm available free chlorine), sodium hydroxide (1 N) and autoclaves (121–134 °C for 1 hour) or a combination of hydrogen peroxide and copper ions neither effectively remove a well-defined α-Syn fibrillar polymorphs adsorbed to different materials commonly used in the laboratory nor disassemble it with efficiency. This is certainly due to the fact that protein particles, made of different proteins, have distinct properties.”[Sci Rep. 2018; 8, 10788]
4. When introduced into the colon, αSynPD seeds would need to go from the colon to the brain:
“In conclusion, we here provide the first experimental evidence that different α-synuclein forms can propagate from the gut to the brain, and that microtubule-associated transport is involved in the translocation of aggregated α-synuclein in neurons.”[Acta Neuropathol. 2014;128(6):805-820]
Additional notes:
PD incidence rate changes varied by age-specific group and by time period in the US.
In 1995, the USPSTF first recommended CRC screening for persons age 50+ years. After 1995, PD incidence decreased for ages under 50 and increased for ages over 50, as show in the graph below.
In 2010, the Affordable Care Act was signed into law. After 2010, PD incidence increased dramatically for ages over 50, but stayed about the same for ages under 50.
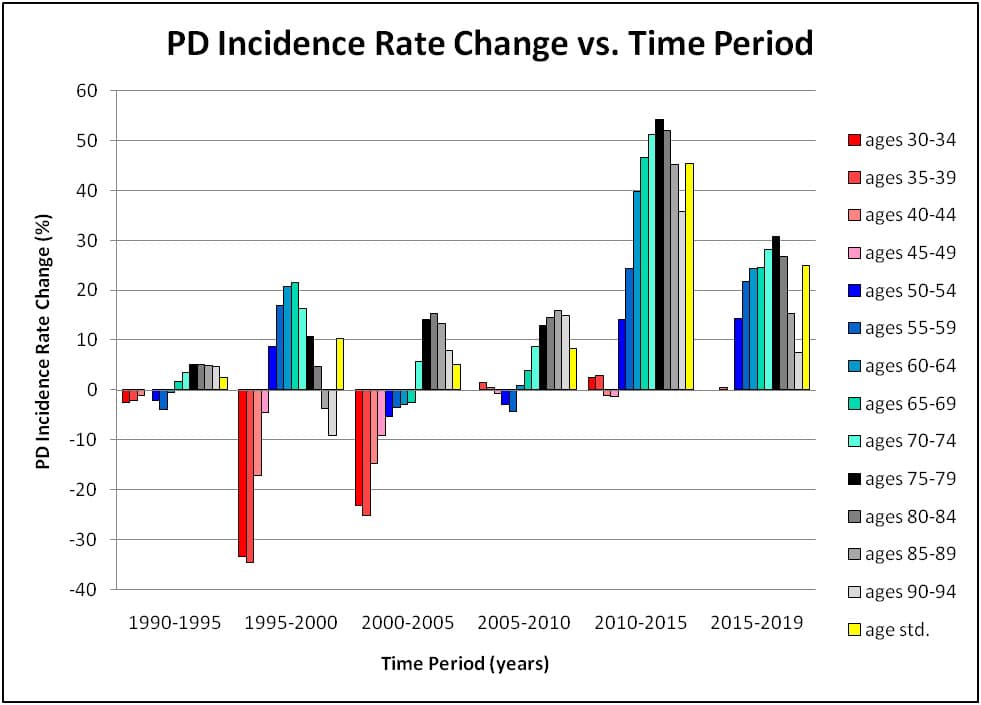
The above graph was generated using PD incidence data from the IHME.
Final notes:
The duration of prodromal PD is unknown.
“Another limitation is that the duration of prodromal PD is unknown.”
“Based upon an overall assessment of the literature, we posited an average prodromal period of 10 years, but this was extremely subjective; the true value may differ considerably.”
The mechanism(s) involved in the initial pathological conversion of α-synuclein is unknown:
“…the identity of causative factor(s) that promote the initial pathological conversion of α-syn into neurotoxic species in PD is largely unsettled.”
A role for an infectious agent has been suggested:
“…the use of preclinical animal models of PD may provide the clearest evidence for or against a role of infectious agents in the etiology of PD.”
Animal models of PD have provided evidence for a role of an infectious agent in the etiology of PD:
“In conclusion, our results demonstrate that α-synuclein can adopt a pathological conformation with infectious and neuroinvasive properties that leads to neuropathology and CNS disease after oral, intravenous, intraperitoneal, or intracerebral delivery which in our opinion qualifies α-synuclein as a prion-like protein.”
My hypothesis:
A colonoscope transfers misfolded αSyn to the colon, where the misfolded αSyn converts the endogenous αSyn to the misfolded conformation, disrupting normal function and causing constipation. The misfolded αSyn then spreads from the colon to the brain via the vagal nerve, as described by Holmqvist et al. (2014).
Since constipation is in the causal pathway, adjustments made during analysis to remove the effect of constipation also would remove the effect of CRC screening colonoscopy.
Constipation is not a confounding variable because it is an effect of the exposure (CRC screening colonocopy) and a factor in the causal pathway of PD.
Restricting the cohorts to include only persons with constipation would remove any effect of constipation without also removing the effect of CRC screening colonoscopy.
References:
(1)
Ritchie, D. L., & Barria, M. A. (2021). Prion Diseases: A Unique Transmissible Agent or a Model for Neurodegenerative Diseases?. Biomolecules, 11(2), 207.
Lauwers, E., Lalli, G., Brandner, S., Collinge, J., Compernolle, V., Duyckaerts, C., Edgren, G., Haïk, S., Hardy, J., Helmy, A., Ivinson, A. J., Jaunmuktane, Z., Jucker, M., Knight, R., Lemmens, R., Lin, I. C., Love, S., Mead, S., Perry, V. H., Pickett, J., … De Strooper, B. (2020). Potential human transmission of amyloid β pathology: surveillance and risks. The Lancet. Neurology, 19(10), 872–878.
Asher, D. M., Belay, E., Bigio, E., Brandner, S., Brubaker, S. A., Caughey, B., Clark, B., Damon, I., Diamond, M., Freund, M., Hyman, B. T., Jucker, M., Keene, C. D., Lieberman, A. P., Mackiewicz, M., Montine, T. J., Morgello, S., Phelps, C., Safar, J., Schneider, J. A., … Frosch, M. P. (2020). Risk of Transmissibility From Neurodegenerative Disease-Associated Proteins: Experimental Knowns and Unknowns. Journal of neuropathology and experimental neurology, 79(11), 1141–1146.
Jaunmuktane, Z., & Brandner, S. (2020). Invited Review: The role of prion-like mechanisms in neurodegenerative diseases. Neuropathology and applied neurobiology, 46(6), 522–545.
Gomez-Gutierrez, R., & Morales, R. (2020). The prion-like phenomenon in Alzheimer’s disease: Evidence of pathology transmission in humans. PLoS pathogens, 16(10), e1009004.
When the risk of PD transmission by colonoscopy is unknown (so probably somewhere between zero and rare) it would seem imprudent to factor this into a decision about having a colonoscopy. We know the risks of colon cancer. One can only conclude that further research is needed.
Hi, Jim! Thank you for sharing your thoughst!